Sports Injuries

Sports injuries of the foot and ankle represent a significant proportion of musculoskeletal trauma encountered in both recreational and elite athletes. As a Consultant Trauma & Orthopaedic Surgeon with extensive experience in managing these conditions, I see daily the profound impact that such injuries can have on mobility, performance, and quality of life.
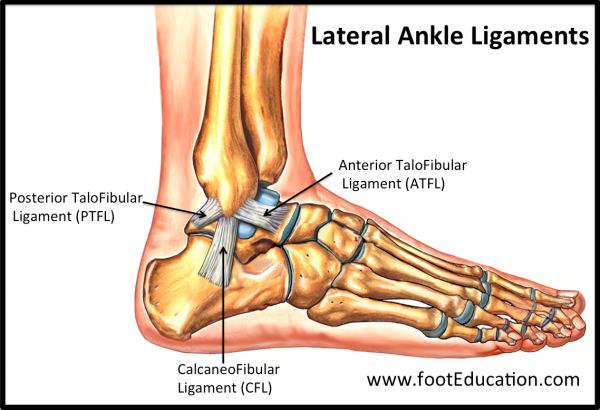
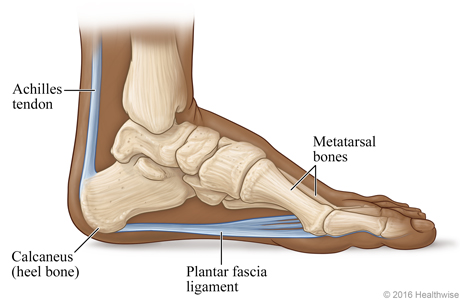
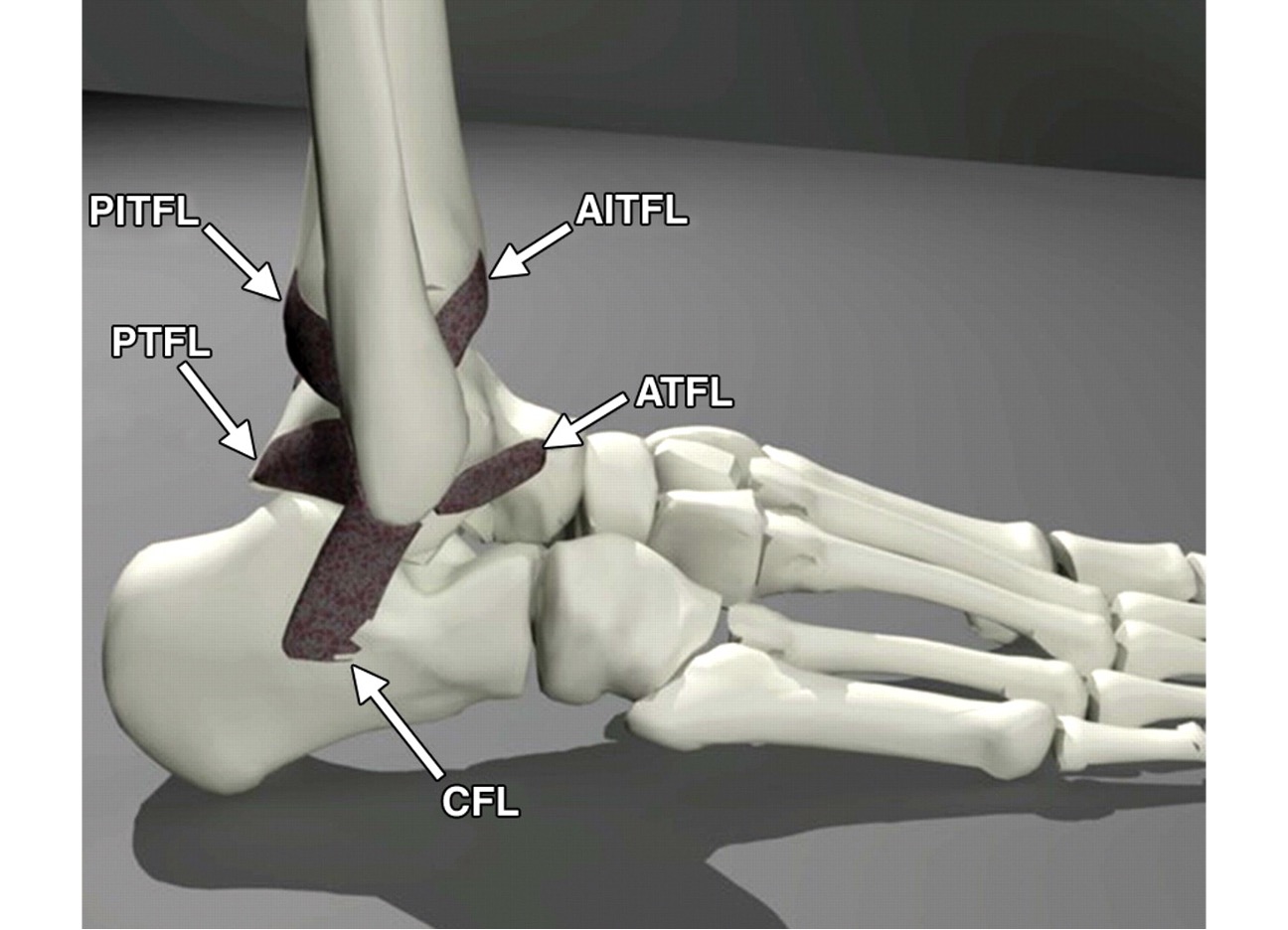
The foot and ankle form a complex biomechanical system comprising 26 bones (hence Twentysix Clinic!), over 30 joints, and numerous ligaments, tendons, and muscles that absorb and transmit forces many times body weight during sporting activity. Acute injuries frequently include ankle sprains, with lateral ligament complex damage being the most common; fractures of the metatarsals, talus, or calcaneus; and Achilles tendon ruptures. Chronic overuse conditions are equally prevalent: plantar fasciitis, Achilles tendinopathy, stress fractures, posterior tibial tendon dysfunction, and osteochondral lesions of the talus.
High-impact sports such as football, rugby, running, and ballet place particular demands on this region, often resulting in syndesmotic injuries, Lisfranc disruptions, or peroneal tendon pathology. Prompt, accurate diagnosis is essential, as untreated or inadequately managed injuries frequently lead to persistent instability, accelerated joint degeneration, and long-term functional limitation.
My practice focuses on precise clinical assessment, state-of-the-art imaging, and evidence-based treatment pathways—ranging from tailored rehabilitation programmes to advanced arthroscopic and reconstructive techniques—aimed at restoring anatomy, stability, and athletic performance with the minimum possible downtime. Early specialist intervention remains the cornerstone of optimal recovery.
Symptoms
- – Stiffness
- – Swelling and inflammation around the joint
- – A feeling of 'going over' on the ankle
- – Pain along a tendon or bone
- – Activity related pain
- Causes and Risk Factors
-
Sports injuries of the foot and ankle typically arise from two principal mechanisms: acute traumatic events and chronic repetitive overload. Sudden inversion or eversion forces during cutting, landing, or collision commonly produce ligament sprains, fractures, and tendon ruptures. Overuse injuries result from cumulative microtrauma, often linked to rapid increases in training volume or intensity.
Key risk factors include inadequate footwear, training on hard or uneven surfaces, intrinsic biomechanical abnormalities such as pes planus, cavus deformity, or ankle instability, and previous injury. Extrinsic contributors encompass age, competitive level, poor conditioning, and insufficient recovery. In my practice, identifying and modifying these factors is fundamental to both treatment and prevention, enabling athletes to return safely to sport with reduced recurrence risk.
- Non-Surgical Treatment
-
The majority of sports-related foot and ankle injuries are successfully managed without surgery. Initial management follows structured protocols, beginning with protection, optimal loading, ice, compression, and elevation (POLICE), followed by early rehabilitation. Physiotherapy focuses on restoring range of motion, proprioception, and peroneal and intrinsic foot strength. Custom orthotics, supportive bracing, and activity modification address biomechanical contributors such as overpronation or instability. In selected cases, image-guided injections of corticosteroid or platelet-rich plasma provide targeted relief. My approach emphasises a personalised, evidence-based programme that accelerates recovery while minimising downtime, allowing most athletes to return to sport without operative intervention.
- Surgical Options
-
When conservative measures fail to restore function or in cases of high-grade instability, displaced fractures, or complete tendon ruptures, surgical intervention is indicated. My practice offers the full spectrum of modern techniques, including arthroscopic debridement and microfracture for osteochondral lesions, anatomic ligament reconstruction for chronic ankle instability, and minimally invasive Achilles tendon repair. Internal fixation of fractures utilises low-profile plates and screws to permit early motion. For Lisfranc or syndesmotic injuries, anatomic reduction and stabilisation are critical. Tendon transfers or osteotomies correct underlying deformity when required. All procedures are performed with meticulous attention to soft-tissue handling and are complemented by individualised postoperative rehabilitation protocols. The goal remains the same: reliable restoration of anatomy and return to pre-injury athletic performance at the earliest safe opportunity.
- Recovery
-
Recovery from foot and ankle sports injuries follows a phased, structured pathway tailored to the specific injury and surgical or non-surgical management. Protected weight-bearing in a walking boot or cast is frequently required for 2 to 6 weeks to allow initial healing while preventing further damage. During this period, attention is given to swelling control, venous thromboembolism prophylaxis, and early range-of-motion exercises where appropriate.
Thereafter, a comprehensive rehabilitation programme commences under the guidance of specialist physiotherapists. This progresses from gait re-education and proprioceptive training to sport-specific drills, strength restoration, and plyometric loading. Regular clinical review ensures safe advancement. Most athletes achieve full return to competitive sport between 3 and 6 months, although complex injuries may require longer. My approach prioritises measured progression to optimise long-term function and minimise re-injury risk.