Heel Pain

Heel pain is one of the most common and often frustrating complaints encountered in foot and ankle practice, particularly among active individuals. As a Consultant Trauma & Orthopaedic Surgeon, I manage a large number of patients whose daily activities and sporting participation are limited by this frequently persistent condition.
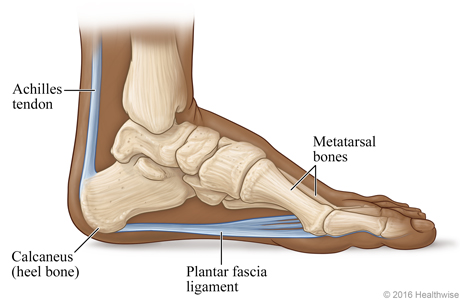
The heel bears significant load during gait and sport, and pain here can arise from several structures, most commonly the plantar fascia, the Achilles tendon insertion, or the calcaneus itself. Plantar fasciitis (fasciopathy) accounts for the majority of cases, presenting as sharp, first-step pain under the heel that improves with activity but often returns after prolonged standing or exercise. Other important causes include insertional Achilles tendinopathy, calcaneal stress fractures, and nerve entrapment.
Patients typically report morning stiffness, activity-related discomfort, and reduced tolerance for running, jumping, or even walking on hard surfaces. Untreated, chronic heel pain can lead to gait alteration, secondary knee or back problems, and substantial loss of quality of life. My practice utilises a structured diagnostic approach with clinical examination, weight-bearing radiographs, and selective ultrasound or MRI to identify the precise source and guide targeted treatment.
Symptoms
- – Sharp first step pain
- – Activity related aching or burning
- – Morning stiffness or tightness
- – Tenderness under heel or foot on direct pressure
- – Pain that worsens towards the end of the day
- Causes and Risk Factors
-
Heel pain, particularly plantar fasciitis, results from repetitive overload of the plantar fascia or Achilles insertion. Key extrinsic factors include sudden increases in training volume or intensity, running on hard surfaces, inappropriate footwear with poor cushioning or arch support, and prolonged standing.
Intrinsic risk factors encompass tight calf muscles, obesity, pes planus or cavus foot types, age over 40, and leg-length discrepancy. Biomechanical issues such as reduced ankle dorsiflexion or excessive pronation further increase stress on the heel. Systemic factors including diabetes, inflammatory arthropathies, and certain medications can also contribute. In athletic populations, a previous history of heel pain or lower limb injury significantly elevates recurrence risk. Early identification of these modifiable factors is essential for effective prevention and management.
- Non-Surgical Treatment
-
Non-operative management is highly effective for the vast majority of heel pain cases and remains the first-line approach. Treatment begins with relative rest, activity modification, and a structured stretching programme targeting the calf and plantar fascia. Night splints, silicone heel cups, and custom orthotics provide mechanical offloading and support.
Physiotherapy emphasises eccentric loading, intrinsic foot strengthening, and gait re-education. Extracorporeal shockwave therapy (ESWT) is a valuable evidence-based adjunct for chronic cases. Simple analgesics or image-guided interventions may be used judiciously for short-term relief. In my experience, a comprehensive six- to twelve-week programme resolves symptoms in over 80–90 % of patients without the need for surgery.
- Surgical Options
-
Surgery is reserved for the small subset of patients with refractory symptoms persisting beyond six to twelve months of optimised non-operative care. For chronic plantar fasciitis, I perform endoscopic or minimally invasive plantar fascia release, often combined with gastrocnemius recession when equinus contracture is present.
Insertional Achilles pathology may require debridement of degenerate tendon, excision of bony spurs, and reattachment using anchors. All procedures are undertaken with meticulous soft-tissue handling to minimise complications such as wound issues or nerve injury. Modern minimally invasive techniques allow smaller incisions, reduced postoperative pain, and faster return to activity. The goal is reliable pain relief while preserving foot biomechanics.
- Recovery
-
Recovery from heel pain follows a measured, progressive pathway. Non-surgical patients typically notice improvement within 6–12 weeks with consistent adherence to stretching, orthotics, and load management. Post-surgical cases involve protected weight-bearing in a walking boot for 2–4 weeks to allow soft-tissue healing.
Thereafter, rehabilitation advances through gentle stretching, progressive loading, and gait retraining under physiotherapy guidance. Return to normal walking is usual by 6–8 weeks, with low-impact activities at 8–12 weeks and full sporting return at 3–4 months, depending on the procedure. Regular clinical review ensures safe progression and addresses any residual stiffness or compensatory issues.